
An everyday story connecting citizens to access health service digitally
It is nearly 10:30 PM. Rahim Mia returns home from his small grocery shop in the village market. He finds his home abnormally quiet and becomes anxious. His only 5-year-old daughter has low grade fever from yesterday and he thought it might be normal cold and cough. In the small tin-shade house, he finds his wife anxiously sitting beside her daughter crying and trying to rinse her head with wet cloth to reduce the temperature.
- ‘What happens’ asks Rahim Mia.
- ‘Temperature is going up from evening and she is not taking anything’ his wife replies.
- ‘Oh my god, where can I find a doctor now in the middle of the night’ Rahim Mia utters with extreme concern about his daughter.
- A bit of silence goes on. Then suddenly his elder son says ‘Papa, I have seen on television promo that by calling the number 16263, anyone can get a doctor any time to discuss health problem. You should call them’.
Rahim Mia took his phone immediately and dialed 16263. The other side replies ‘I am Dr Salma. How can I help you?’ After talking few minutes with him in empathy, the doctor provides advice to him to buy and use paracetamol suppository to reduce her temperature. He also advises to give her more fluid to drink. Doctor continues, “It will be wise to bring her to the nearest Upazila Health Complex next morning. I am sending the prescription by SMS. Please show the SMS to a medicine shop to get the paracetamol suppository.”
The above features one of the current pictures of Bangladesh’s Digital Health. “16263” is the short code of the one-stop integrated national health call center, known as Shaystho Batayon 16263. It gained good popularity since its launch in September 2015. Any person across the country can call the number anytime 24/7 and gets for free instant services like (i) doctors’ advice and prescription; (ii) reservation of ambulance; (iii) provision of health Information; (iv) receipt and resolution of client complaints about any public or private health care provider; and (v) coordination and addressing emergency health situation with help national emergency call center 999. People also can get access to health service through telemedicine, text message broadcast on health information and awareness, and lodging complaints through text message or telephone call.
A short list of digital health services
Bangladesh, a developing country in the South-East Asia, harnessed impressive rollout of eHealth in its public health sector. As the world’s first nation to announce “Digital Bangladesh 2021” vision in 2009, the country made mind boggling progress in all areas of eHealth, viz., connectivity; data gathering, evidence generation and response; telemedicine; public accountability; health call center; text message broadcast for citizens’ and health staffs’ awareness and communication; shared health record for universal life time EHRs and hospital automation; human resource management and information system; eFiles; health facility licensing and renewal system; routine weekly video review meeting with over hundred places with the all health managers across the country; electronic monitoring of office attendance, equipment functionality, supplies, service utilization and complaint redressal; social media boosting staff motivation and skill development, and health educating of public; eye catching real time public dashboard as an open government policy to keep people informed and ensure accountability, etc.
District Health Information Version 2 (DHIS2) – Bangladesh is the world’s largest and best deployment
A 2014 publication of the German Federal Ministry of Economic Development titled “A Quiet Revolution Strengthening the Routine Health Information System in Bangladesh” describes in good detail Bangladesh’s glorious journey on improving routine health information system with use of District Health Information System version 2, an opensource public health data gathering database software which is warmly acclaimed globally. This book is available on the Internet for freed download at this URL: https://health.bmz.de/ghpc/case-studies/A_Quiet_Revolution/index.html. Since 2009, Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) supported the Management Information Systems (MIS) of the ministry’s Directorate General of Health Services to introduce DHIS2. Almost all of the country’s health facilities and health organizations, both public and private, and all public sector community health workers in Bangladesh use this database software for pushing and pulling data and reports from this system. The total number of end users is about 50,000 via mostly through wireless modems, which gives the MOHFW the status of Bangladesh’s single largest mobile subscriber. The gigantic size of DHIS2 users across vast geographical domains and widely diverse nature of user types, Bangladesh is recognized as the world’s largest and best deployment of DHIS2. Introduction of DHIS2 in Bangladesh has set the momentum of eHealth data standardization and interoperability, which the country believes and practices in all of its software and database development. This enthusiasm inspired Bangladesh to lead a World Health Assembly a resolution A64.R24 on eHealth Standardization and Interoperability in 2013. Bangladesh has built local capacity to maintain, develop, promote and expand the use of DHIS2 and overall health information system (HIS) governance. All the health sector partners have been brought together under the leadership of DGHS to use its eHealth resources including DHIS2 as common property and to invest in for further development. This collective vision resulted in continued thriving and expansion of DHIS2 and other eHealth resources despite the GIZ assistance ended in 2015.
A dissection of the DHIS2 platform in Bangladesh
Use by almost all stakeholders as data repository, DHIS2 in Bangladesh has been prominent as the national health data warehouse. It is thus helping in bridging data gap between the fragmented data systems while bringing together information from various sources in a common place. It has rich data mining functions enabling generation of reliable and accurate data for evidence-based decision-making, and planning and monitoring of health interventions aimed to achievement of health-related SDGs.


DHIS2 in disease surveillance
The Institute of Epidemiology, Disease Control and Research (IEDCR), the country’s disease surveillance focal point uses DHIS2 for feeding, processing, analyzing and reporting data for disease surveillance. Special mention needs Kala-Azar (Visceral ) elimination target achieved by Communicable Disease Control Program of DGHS in 2018. DHIS2 tracker was used for this purpose, which tracked each individual patient of Kala-Azar for treatment and follow-up including to see any adverse drag reaction. A similar ongoing program is tracking cervical and breast cancer patients screening, treatment and follow-ups jointly by MIS-DGHS and Bangabandhu Sheikh Mujib Medical University (BSMMU).
Human Resource Information System (HRIS)
A complete solution of human resource management for entire MOHFW and for capturing health workforce data from the non-state health sector, the ministry’s HRIS is another key milestone of Bangladesh’s digital health. Developed and anchored by MIS-DGHS, the HRIS is comprised of 4 registries, namely, geo-location registry, facility registry, sanctioned post registry, and provider registry. All human resource-related functions, including new appointment, posting, biometric office attendance, transfer, promotion, deputation, leave, annual confidential report, disciplinary action, etc. can be maintained, processed and reported through this wonderful electronic platform.
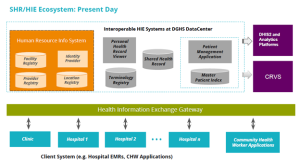
Citizen’s life-time electronic health record and hospital automation
Purposefully designed for gradually moving to a national electronic archive of citizens’ life-time portable electronic health records and using them real-time whenever patient encounters will occur anywhere in the country, the MIS-DGHS also developed an ambitious Shared Health Record (SHR) project. In this case, patients do not need to carry personal health file, and the doctor or health facility can retrieve and work on the individual electronic health file on demand. This has been made possible through an electronic gateway called Health Information Exchange (HIE) allowing transport of data between health facilities and healthcare providers. Adequate provisions of permission, credentials, privileges, confidentiality and data security are in-built in the system. Being piloted in few hospitals, SHR is being rolled out in the country.

Hospital automation
In promoting and scaling of digital health, the MOHFW of Bangladesh also gave preference to open source non-proprietary software. The reason is for making software acquisition affordable and establishing ownership on the system. So, the well-known hospital management system called OpenMRS (Open Medical Record System) has been collected and tremendously improved to make a robust and complete solution for hospital automation and build national electronic hospital networking system. The Bangladeshi version of OpenMRS in termed as OpenMRS+ as it represents a composite modules of OpenMRS, OpenERP(now odoo), OpenELIS and dcm4chee. The OpenMRS+ is tied with the SHR system, so that both can work interactively through the Open HIE in transportation of patients’ electronic files to central repository for storing an updated version and to the health facilities or providers who require them. A number of hospitals are using the system. Others, both public and private, are being encouraged to take a free copy the software to join in the national hospital automation system network.
Public data dashboard and remarkable health system strengthening tool
The DGHS, on its web portal, host a very rich, elegant and integrated dashboard, which can be accessed through the URL www.dghs.gov.bd and then clicking on Dashboard. The dashboard pools data on real time in a common place from all the existing databases. For this purpose, besides using DHIS2 analytics tools, the dashboard also uses potential renowned business intelligence (BI) tools named Tableau, Jaspersoft, Google Chart API and High Chart API for in-depth analysis and visualization.

The dashboard is open to public and is also used as Health System Strengthening (HSS) tool for all government health organizations’ performance, monitoring, measurement, motivation and recognition. All the required activities of the health systems and organizations have been listed in database system in each category of 6 building WHO building blocks. They have been scored through giving appropriate weightage under an agreed measurement scale. Whenever any organization performs and activity and this recorded in the system, it is automatically scored depending on the amount and quality of the output. Scores for all activities performed are aggregated and summarized. The HSS tool evaluates performances of all organizations and identifies the top performers in several categories for health minister’s national award. A gala annual event is held where the awards are given to eligible organizations. The HSS tool is making measurable and visible improvement in the health system. Because of the significant strength of the system, the HSS tools is being supported by WHO, UNICEF, HISP Bangladesh and ICDDRB.

It is better to further explain how the HSS tool works. It is based on WHO’s health system and the result chain analytical frameworks adopted with the local context. Performance indicators have been defined at input, output and outcome levels, and to some extent, at the impact level for facilities and community health services. In total, health system champions are identified through using four different tools. The first one, online measurement tool in which score is automatically filled in from the routine health data provided by the health facilities through different database system; mainly DHIS2 and HRIS. The second tool is onsite physical inspection using structured data collection forms to validate the claims made by health facilities in the routine data provision system. The third tool uses a further physical inspection by an independent team of assessors on the short-listed facilities. The fourth tool is a patient satisfaction survey. Each tool generates scores against individual health facility. The scores gathered from all the four tools are combined to identify the champions for health minister’s award.
Online local health bulletins
Some people do not feel comfort in directly digging into data. They prefer a readymade way to get all data summarized in bulletin form in one place. It may also be wonderful to organize data in a printable standard format so that respective facility or interested viewers can print it in a book form. This idea helped to innovate Local Health Bulletins. The local health bulletins are really the brilliant creation of our meritorious software development team, which empowered the dashboard visitors to create local health bulletins with updated data on their choice for one or more of hundreds of health facilities on real time. The intelligent tool mines data across all the integrated databases and compiled them in book format for easy to understand viewing and for printing.
Civil Registration and Vital Statistic (CRVS)
The SDG 16.9 puts emphasis for legal identity for every citizen in each country from birth to death to enable citizens enjoy their due human rights and privileges. CRVS is for establishing this vision. The importance of CRVS is being viewed seriously from the report of the UN Commission on Information and Accountability of Women and Child Health 2010. Bangladesh revitalized it’s CRVS, being motivated from this report, with WHO’s technical assistance since 2012. The government has a whole-of-government approach to establish CRVS in Bangladesh in a broader perspective with additional domains with a nomenclature of CRVS++. From the digital health perspective, an Enterprise Architecture (EA) has been developed. MOHFW started to notify birth and death events taking place in the community and health facility with cause of death to the Office of the Registrar General. Therefore, the SOP is now under the process of being revised. Verbal autopsy in the community and Form 804 in the hospital are used to identify the cause of death. International standard medical certificate of cause of death (MCCOD) has been introduced using Startup Mortality List (ICD-10- SMoL) as well as ICD10. A MCCOD module has been developed and integrated with the national DHIS2 platform.

Telemedicine
Started in 2009 from only 8 telemedicine centers, currently telemedicine service is being provided from about 100 centers spanning all types of hospitals, viz., medical college hospitals, district hospitals and sub-district hospitals, across the country. The telemedicine centers are equipped with tele-gadgets, like tele-stethoscope, tele-ECG, tele-microscope, tele-glucometer, etc. and they also have high-quality cameras, big screen monitors, computers, etc.
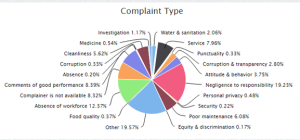
Citizen’s grievances management system
A complaints and suggestions management system has been launched in 2012. The system is like this. In each of the 739 public hospitals and health organizations, there is a display board mounted on the wall of a prominent place. The display board describes how to send, through SMS, complaints about the quality of services or suggestions for improvement thereof. As soon as a SMS is sent, a web-server instantly receives, processes and display it on the web portal for public viewing. One dedicated person follows up each text message and contact both with the message sender and complainant and resolves the issue with full feedback to the complainant.
Monitoring nationwide staff attendance through biometric system
Absenteeism of service providers in the health facilities particularly in the rural and remote areas is not uncommon in Bangladesh, as it happens also in many other countries. To address the problem, the MOHFW placed remote biometric time-attendance machines in all the public hospitals. Personnel and staff need to touch with finger the respective health facility machine(s) during arrival and departure. All the touch information is accumulated in the central server from where local and national authority as well as general public can view the staff attendance situation through web portal. The authority can see every detail of the information for individual staff. The MOHFW is now working to link the attendance with the career plan and incentives mechanism of the personnel and staff.
Video-conferencing system
Every first, third and fifth Monday of a month at 9:30 am, the Director General of Health Services (DG-HS) routinely meets with all his 8 divisional and 64 district health managers. Every third Monday of a month, about 500 sub-district health managers also join in the same meeting. Every second and fourth Thursday at the same time, the DG-HS meets all the principals of medical colleges and directors of all the postgraduate institute hospitals and medical college hospitals. Every Tuesday the personnel and staffs of the telemedicine centers join in meeting. All of these happen through video conference. Nobody needs to travel outside of their office premise. These routine meetings discuss the management issues, review the progress towards the health targets, and disseminate general instructions, explanations, guidelines, etc. Large, medium or small group meetings, seminars, trainings, emergency health management (viz., in case of road or building accidents, fire incidences, natural disasters, etc.) are also performed through video conference. The value of the video conference meetings are manifolds, beginning from improvement of health managers’ vocabulary and communication skills, creation of positive environment of supportive supervision, and closing the relationship gaps between the top and bottom managers.

Digital displays for public viewing and education
The MOHFW recently installed several large displays in different location of Dhaka city to create public awareness on health, nutrition and family planning, and to disseminate important information and success stories of health. Video clips, PowerPoint slides or Microsoft Office files are also shown. The unique feature of these displays is that these are remotely controlled from a common location at DGHS pushing the data through Internet.
Big data, artificial intelligence and robotics
An innovative environment for digital health development exists at the MIS-DGHS which is the hub of digital health program of Bangladesh government. When there is a sea of data at the central data repository of DGHS growing at a phenomenal rate every day, the DGHS is now looking for big data analysis, artificial intelligence and machine learning platform to do something more. Robotics and bots can be a potential area to replace the need of human workforce for which the ministry has acute crisis. In February 2019, the MOHFW therefore held the first International conference in Dhaka on Big Data for Health. The DGHS is keen to collaborate with potential partners to work in this new area.
Conclusion
The achievement of digital health in Bangladesh is really mind boggling and exciting. The stimulus and inspiration came from top level national policy of Digital Bangladesh Vision 2021. The Honorable Prime Minister of Bangladesh Sheikh Hasina is futuristic and visionary. As she aspires for ambitious health goals not to fail in SDGs, so she aspires for highest possible attainment of Digital Bangladesh as a whole. The world has recognized her contributions. She received many globally distinctive awards in diverse fields, however, most of them were for health. One health award was United Nations Digital Health Award 2011. From this strong political support from the highest level, the digital health players of Bangladesh always remain optimistic for brighter and brighter digital health future in Bangladesh.
Few additional references: